COVID-19: Vaccines (Part 3 of 3): You’re Safe if You’re Vaccinated
by
Columbia University Professor Emeritus, Dr. David Figurski
presented by
Donna O’Donnell Figurski
(Disclaimer: The World Health Organization <WHO> has officially named the new coronavirus as SARS-CoV-2 and the disease it causes as COVID-19. Because the majority of people, including much of the press, commonly refer to the virus as “COVID-19,” to avoid confusion, I use COVID-19 as the name of the virus.)
David H. Figurski, Ph.D & Survivor of Brain Injury
Some things people need to know about vaccination and life after vaccination.
If you’re healthy, you don’t need a booster, but it won’t hurt to get it. Donna and I will get the booster because we’re in the senior demographic, and our immune systems may have declined somewhat.
Vaccinated people can get infected, but their disease will be mild or asymptomatic. There is no such thing as a “breakthrough infection.” All vaccines allow infection, but prevent severe disease.
Because vaccination doesn’t prevent infection, we definitely don’t want to infect any of the as-yet-unvaccinated children. We always wear our masks around children and try to keep a distance between them and us.

vaccine Stop Coronavirus, covid – 19 , China, Wuhan, Danger, vector Illustration.
For the reasons I discuss below, virologists in my former department at Columbia say the vaccines will protect you from all the variants we know about – despite all the hysteria.
Columbia virologist Vincent Racaniello continues to emphasize that there are no data to support increased transmissibility of any variant. Delta might be widespread for any one of a number of possible reasons.
All the US vaccines are safe. Because of them, my fears of hospitalization and death are gone.
But we still may be susceptible to getting Long COVID (see below). (There aren’t enough data yet on whether vaccinated people can still get Long COVID.) The reason this is an issue is because Long COVID can apparently be brought on by a mild infection.
 Even though we’ve been vaccinated, we are still being careful. We try to mix with vaccinated people only. We try to avoid people and places that might be hot spots for infection. We only eat on restaurant patios; we never eat inside. We still practice social-distancing when we can, and we still wash our hands thoroughly and use disinfectant if we can’t wash our hands.
Even though we’ve been vaccinated, we are still being careful. We try to mix with vaccinated people only. We try to avoid people and places that might be hot spots for infection. We only eat on restaurant patios; we never eat inside. We still practice social-distancing when we can, and we still wash our hands thoroughly and use disinfectant if we can’t wash our hands.
But we have also relaxed several things. Donna now goes into stores, but she always wears her mask. We’ve traveled by car, so we have stayed in motels. Although we don’t eat inside, we have walked through several restaurants with our masks on. Also, we’ve eliminated some precautions with our mail and our food packages.
You can stop here.
If you want more detail, the following is an easily understood explanation of what the vaccines do and why they’re so protective.
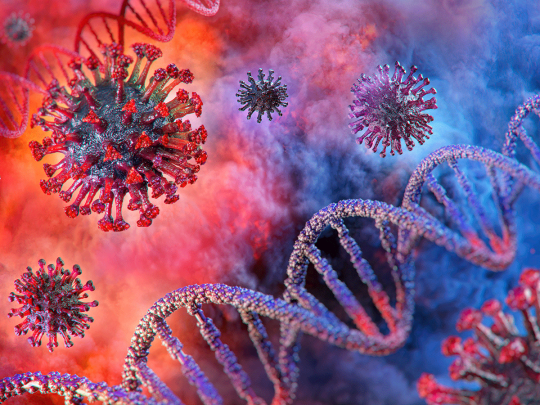
All the currently approved US vaccines are directed to one viral protein: the Spike protein. Spike proteins decorate the virus coat. They are responsible for allowing the virus to bind to a protein (ACE2) on the surface of lung cells. Because the viral-encoded Spike protein and the host-encoded ACE2 protein bind to each other, the virus can bind to the lung cell and get inside to start an infection. This means the lung cell will be hijacked and reprogrammed to make more virus particles. Each infected cell will release thousands of new virus particles. They can then attach to more lung cells. And the cycle repeats. You can easily see how a virus can quickly overwhelm its host animal.
(Incidentally, the Spike protein probably got its name because pictures (electron micrographs) of the virus show that it resembles a “mace,” a weapon used in medieval times. The head of the mace had spikes which did the damage. Similarly, the coronavirus particle is coated with “spikes.” They are made from trimers (assemblies of three copies of a single kind of protein) of the Spike protein. Coronavirus definitely got its name from pictures. Several Spike protein trimers on the surface of each virus particle make the virus look like a cartoon-drawing of the sun. The spikes on the virus look like the “corona” of the sun.)
Antibodies work by binding to the Spike protein and preventing the Spike protein from binding the lung cell’s ACE2 protein. As a result, the virus can’t bind a lung cell to start an infection.
All proteins are made up of a series of amino acids linked end to end. The Spike protein has 1273 amino acids. The sequence and types of amino acids (of which there are 20) determine the property and the folding of the Spike protein. The proteins are molecular machines. There are tens of thousands of different proteins in the human body – each one doing a unique job. The virus-encoded Spike protein is the viral machine that makes it possible for the SARS-2 coronavirus to infect lung cells.
Of the 1273-amino acids in Spike protein, only a few amino acids form the binding domain that allows binding of Spike protein to ACE2. Antibodies that bind to this binding domain of Spike protein inactivate the Spike protein and prevent the virus from infecting lung cells. Such antibodies are called “neutralizing antibodies.” The purpose of the vaccines is to stimulate the production of antibodies to the entire Spike protein, some of which will be neutralizing antibodies that can block infection. In other words, the neutralizing antibodies are a subset of all the antibodies produced that bind to the Spike protein. Because the Spike protein has lots of amino acids and lots of domains, it will stimulate lots of different antibodies that will bind the Spike protein, but only those that bind to the Spike domain that binds ACE2 are neutralizing antibodies. Only they will prevent the ability of the virus particles to bind to lung cells and get in.
The sequence of the 1273 amino acids in the Spike protein can also be seen as several smaller sequences of amino acids. Some small sequences of amino acids can fold properly and stimulate the formation of specific antibodies directed against that small domain. So most of the Spike-protein-specific antibodies bind the Spike protein at other places and do not block the ability of the virus to bind to and infect lung cells. The most relevant domain is the sequence of amino acids needed to form and fold properly so that Spike protein (and therefore the virus) can bind the lung cell’s ACE2 protein. Antibodies to that domain prevent binding of the virus to lung cells. These are the antibodies of interest – the so-called “neutralizing” antibodies. In fact, scientists are thinking of using only the amino acids that allow the proper structure of the ACE2-binding domain to form. If a vaccine can be made from the ACE2-binding domain only of the Spike protein, then maybe more neutralizing antibodies would be made, and the vaccine might even be better at preventing disease.
Some variants are known to bind the neutralizing antibodies less well. The virus has “seen” many vaccinated people, so there is “pressure” for the virus to change to ensure its survival. Some altered viruses randomly arise with slight changes, like differences in the amino acid used at a certain position of the Spike protein. (There is a reason why Nature allows DNA and RNA replication to make some random, but very rare, errors.) Some changed (=mutant=variant) viruses are still able to form a domain of Spike protein that can bind ACE2 yet evade some of the neutralizing antibodies that block the original Spike protein. Such changed viruses may do better and eventually become predominant. So random errors in replication can lead to viruses that have some ability to resist neutralizing antibodies, yet still bind to lung cells to start infection. These are what we are calling “variants.” Because the change increased the virus’ chance of escaping neutralizing antibodies, it survives better. The arising of variants is evolution that we can see happening in real time.
But we got lucky! Some of the variants (like Delta) may escape some neutralizing antibodies. But we are still protected! The Spike protein also stimulates killer T cells, an important arm of the immune system that is usually ignored.
The killer T cell arm of the immune system is as potent as the more commonly known antibody arm. Not every protein has sequences that can instruct killer T cells, but Spike protein does. When a cell makes proteins, a small fraction of each protein being synthesized is chopped up, and small fragments of that protein are displayed on the surface of the cell. The immune system has a way to instruct a killer T cell to kill any cell making a foreign protein (that is, one not made by the human body). A killer T cell that has “learned” to recognize a fragment of Spike protein on a cell’s surface will kill the cell making it because that cell is considered to be making virus.
And that’s not all! The antibody arm of the immune system is less potent in the variants, but the killer T cell arm is completely unaffected. Not only that, but, whereas a variant resistant to the antibodies can affect an entire population, because of mechanism, it is impossible for a variant resistant to killer T cells to spread beyond a couple of individuals in the worst-case scenario.
Bottom line: All the Spike-protein-based vaccines we know about (Pfizer-BioNTech, Moderna, J&J, and the UK’s Oxford-Astra Zeneca) are protective beyond expectations. You’re safe if you’re vaccinated.
Get Your Copy Now
Read It! Review It!
Click Links under Book

PAPERBACK! Read it Now! e-BOOK! Read it Now!
Stay Safe and Healthy!
Clip Art compliments of Bing.com.
(Photos compliments of contributor.)
As I say after each post:
Please leave a comment by clicking the blue words “Leave a Comment” below this post.
Feel free to follow my blog. Click on “Follow” on the upper right sidebar.
If you like my blog, share it intact with your friends. It’s easy! Click the “Share” buttons below.


 A recent paper submitted by an Israeli group showed there is a significant reduction (an appropriately conservative conclusion for data that showed 0 cases of long COVID) if a person was vaccinated before getting infected. In contrast, with no vaccination, about half of hospitalized COVID-19 patients will get long COVID. Vaccination after getting COVID-19 helps: Vaccination within 30 days of COVID-19 infection helps reduce the incidence of long COVID significantly. Getting vaccinated 30-60 days after COVID-19 infection helped, but not as much as within 30 days. Getting vaccinated after 90 days post COVID-19 infection does not help.
A recent paper submitted by an Israeli group showed there is a significant reduction (an appropriately conservative conclusion for data that showed 0 cases of long COVID) if a person was vaccinated before getting infected. In contrast, with no vaccination, about half of hospitalized COVID-19 patients will get long COVID. Vaccination after getting COVID-19 helps: Vaccination within 30 days of COVID-19 infection helps reduce the incidence of long COVID significantly. Getting vaccinated 30-60 days after COVID-19 infection helped, but not as much as within 30 days. Getting vaccinated after 90 days post COVID-19 infection does not help.


 Columbia virologist Dr. Vincent Racaniello discusses the “mildness” of the omicron variant with Dr. Daniel Griffin, a New York physician in Columbia’ s Department of Infectious Diseases.
Columbia virologist Dr. Vincent Racaniello discusses the “mildness” of the omicron variant with Dr. Daniel Griffin, a New York physician in Columbia’ s Department of Infectious Diseases. 
 Vaccination stimulates your adaptive immunity, so the antibodies and T cells are ready before infection.
Vaccination stimulates your adaptive immunity, so the antibodies and T cells are ready before infection. In some cases, there were several weeks of good health. But weeks or months later, they showed new symptoms. (Adult symptoms include fatigue; fever; cough; sore throat; chest pain; shortness of breath; neurocognitive problems with memory, concentration, processing, or finding words; diarrhea; headaches; insomnia; dizziness; heart palpitations; abdominal cramps, rashes; tinnitus; joint pain; depression; and anxiety.) The symptoms may last weeks or months, and some people still have symptoms after several months.
In some cases, there were several weeks of good health. But weeks or months later, they showed new symptoms. (Adult symptoms include fatigue; fever; cough; sore throat; chest pain; shortness of breath; neurocognitive problems with memory, concentration, processing, or finding words; diarrhea; headaches; insomnia; dizziness; heart palpitations; abdominal cramps, rashes; tinnitus; joint pain; depression; and anxiety.) The symptoms may last weeks or months, and some people still have symptoms after several months. I haven’t seen the data, but I suspect that the 10-13% number came from people who either had an obvious symptom or tested positive. If we include the number of asymptomatic infections, the percentage of infected children who get long COVID will likely go down significantly. If you and your children are using masks and social-distancing, then you’re already at a low risk of even getting infected.
I haven’t seen the data, but I suspect that the 10-13% number came from people who either had an obvious symptom or tested positive. If we include the number of asymptomatic infections, the percentage of infected children who get long COVID will likely go down significantly. If you and your children are using masks and social-distancing, then you’re already at a low risk of even getting infected. 





 Is the President contagious? We can’t say without knowing his test results. Dr. Griffin considers a patient virus-free if that person has two negative tests on two consecutive days. Otherwise, a person is considered to be potentially contagious for 20 days. Since the doctors are permitting the President to hold rallies, I assume he is not thought to be contagious.
Is the President contagious? We can’t say without knowing his test results. Dr. Griffin considers a patient virus-free if that person has two negative tests on two consecutive days. Otherwise, a person is considered to be potentially contagious for 20 days. Since the doctors are permitting the President to hold rallies, I assume he is not thought to be contagious.

 Cytokines are molecules released by some cells that cause an action by other cells. When certain immune system cells sense a problem (like a virus-infected cell), they release cytokines to get other immune cells to multiply, to make attack molecules, or to come and help eliminate the cause of the problem. Normally, the immune system works well, but sometimes the immune system overreacts and causes severe problems or even death. “Cytokine storm” refers to an overreaction by the immune system. A steroid (for example,
Cytokines are molecules released by some cells that cause an action by other cells. When certain immune system cells sense a problem (like a virus-infected cell), they release cytokines to get other immune cells to multiply, to make attack molecules, or to come and help eliminate the cause of the problem. Normally, the immune system works well, but sometimes the immune system overreacts and causes severe problems or even death. “Cytokine storm” refers to an overreaction by the immune system. A steroid (for example,  dexamethasone, which the President was given) is effective because it will dampen the immune response, a potentially beneficial effect when the immune system is overreacting. But, dexamethasone is considered harmful if the drug is not needed. (For example, dexamethasone is not given in Week 1 <the viral phase> because a normally functioning immune system is needed to reduce the amount of virus in the body.)
dexamethasone, which the President was given) is effective because it will dampen the immune response, a potentially beneficial effect when the immune system is overreacting. But, dexamethasone is considered harmful if the drug is not needed. (For example, dexamethasone is not given in Week 1 <the viral phase> because a normally functioning immune system is needed to reduce the amount of virus in the body.) dexamethasone should only be given to patients with moderately severe or serious COVID-19 disease. The White House acknowledged that the President received oxygen before he was taken to Walter Reed. Supplemental oxygen is consistent with the President’s being given dexamethasone. Dr. Griffin said that oxygen, if needed, is usually given in Week 2, further indicating that the President’s infection may have started several days before Friday. October 2nd.
dexamethasone should only be given to patients with moderately severe or serious COVID-19 disease. The White House acknowledged that the President received oxygen before he was taken to Walter Reed. Supplemental oxygen is consistent with the President’s being given dexamethasone. Dr. Griffin said that oxygen, if needed, is usually given in Week 2, further indicating that the President’s infection may have started several days before Friday. October 2nd. Doctors have found that COVID-19 has a third phase – a “clotting phase,” which starts at the end of Week 2 and extends at least through Week 3. COVID-19 infection can trigger clots, which can sometimes (albeit rarely) lead to strokes. Aspirin is routinely given at the end of Week 2 because it helps prevent clotting. Some patients had already been discharged from the hospital (having had two negative COVID-19 tests over two consecutive days and having agreed to self-quarantine for 14 days as a precaution) when a problem-clot occurred.
Doctors have found that COVID-19 has a third phase – a “clotting phase,” which starts at the end of Week 2 and extends at least through Week 3. COVID-19 infection can trigger clots, which can sometimes (albeit rarely) lead to strokes. Aspirin is routinely given at the end of Week 2 because it helps prevent clotting. Some patients had already been discharged from the hospital (having had two negative COVID-19 tests over two consecutive days and having agreed to self-quarantine for 14 days as a precaution) when a problem-clot occurred.









Recent Comments